ГастроМентор - симулятор гастро- и колоноскопии


Навыки
- Гастроскопия
- Колоноскопия
- Гибкая сигмоидоскопия
- Эндоскопическая ультрасонография
Характеристики
- Подвижная платформа на колесах
- Сенсорный экран 24 дюйма
- Использование реальных адаптированных колоноскопа и дуоденоскопа
- Имитаторы вспомогательных эндоскопических инструментов
- Непревзойденная точность отслеживания движений инструментов
- Реалистичная обратная тактильная связь
Обучающий контент
- Обширная библиотека обучающих модулей от базовых до продвинутых
- 3D-карта и виртуальный инструктор обеспечивают динамичную обратную связь и облегчают ориентирование и понимание анатомии
- Шкала боли виртуального пациента
- Единственный симулятор для освоения практических навыков EUS (эндоскопической ультрасонографии)
- Симулятор с доказанной эффективностью, валидированный в более чем 40 исследованиях по всему миру
- Дидактические материалы включают интерактивные инструкции и готовые обучающие курсы
МенторЛерн
Уникальная система управления учебным процессом на всех симуляторах Simbionix
Подробнее про МенторЛерн
|
SXGIG |
Симулятор ГастроМентор в комплекте с базовыми модулями
|
|
SXGI/Bap |
Набор дополнения симулятора ГастроМентор модулями по бронхоскопии (базовый пакет):
|
SX-PWPU Годовое постгарантийное обслуживание симулятора
Validity evidence for a new portable, lower-cost platform for the fundamentals of endoscopic surgery skills test.
Mueller CL1, Kaneva P, Fried GM, Mellinger JD, Marks JM, Dunkin BJ, van Sickle K, Vassiliou MC.
Author information
Steinberg-Bernstein Centre for Minimally Invasive Surgery, McGill University Health Centre, Montreal, QC, Canada
Surg Endosc. 2015 Jul 3. [Epub ahead of print]
BACKGROUND: The fundamentals of endoscopic surgery (FES) examination measures the knowledge and skills required to perform safe flexible endoscopy. A potential limitation of the FES™ skills test is the size and cost of the simulator on which it was developed (GI Mentor™ II virtual reality endoscopy simulator; Simbionix LTD, Israel). A more compact and lower-cost alternative (GI Mentor™ Express) was developed to address this issue. The purpose of this study was to obtain evidence for the validity of scores obtained on the Express platform, so that it can be used for testing.
STUDY DESIGN: General surgery residents at various levels of training and practicing endoscopists at five institutions participated. Each completed the five FES tasks on both simulator platforms in random order, with 3-14 days between tests. Scores were calculated using the same standardized computer-generated algorithm and compared using Pearson’s correlation coefficient.
RESULTS: There were 58 participants (mean age 32; 76 % male) with a broad range of endoscopic experience. The mean (95 % confidence interval) FES scores were 72 (67:77) on the GI Mentor™ II and 66 (60:71) on the Express. The correlation between scores on the two platforms was 0.86 (0.77:0.91; p < 0.0001).
CONCLUSION: There is a high correlation between FES manual skills scores measured on the original platform and the new Express, providing evidence to support the use of the GI Mentor™ Express for FES testing
Evaluation of Two Flexible Colonoscopy Simulators and Transfer of Skills into Clinical Practice
Gomez PP1, Willis RE2, Sickle KV2
1Department of Surgery, University of Texas Health Science Center at San Antonio, San Antonio, Texas. Electronic address: gomezpp@uthscsa.edu.
2Department of Surgery, University of Texas Health Science Center at San Antonio, San Antonio, Texas.
J Surg Educ. 2014 Sep 16. pii: S1931-7204(14)
INTRODUCTION: Surgical residents have learned flexible endoscopy by practicing on patients in hospital settings under the strict guidance of experienced surgeons. Simulation is often used to “pretrain” novices on endoscopic skills before real clinical practice; nonetheless, the optimal method of training remains unknown. The purpose of this study was to compare endoscopic virtual reality and physical model simulators and their respective roles in transferring skills to the clinical environment.
METHODS: At the beginning of a skills development rotation, 27 surgical postgraduate year 1 residents performed a baseline screening colonoscopy on a real patient under faculty supervision. Their performances were scored using the Global Assessment of Gastrointestinal Endoscopic Skills (GAGES). Subsequently, interns completed a 3-week flexible endoscopy curriculum developed at our institution. One-third of the residents were assigned to train with the GI Mentor simulator, one-third trained with the Kyoto simulator, and one-third of the residents trained using both simulators. At the end of their rotations, each postgraduate year 1 resident performed one posttest colonoscopy on a different patient and was again scored using GAGES by an experienced faculty.
RESULTS: A statistically significant improvement in the GAGES total score (p < 0.001) and on each of its subcomponents (p = 0.001) was observed from pretest to posttest for all groups combined. Subgroup analysis indicated that trainees in the GI Mentor or both simulators conditions showed significant improvement from pretest to posttest in terms of GAGES total score (p = 0.017 vs 0.024, respectively). This was not observed for those exclusively using the Kyoto platform (p = 0.072). Nonetheless, no single training condition was shown to be a better training modality when compared to others in terms of total GAGES score or in any of its subcomponents.
CONCLUSION: Colonoscopy simulator training with the GI Mentor platform exclusively or in combination with a physical model simulator improves skill performance in real colonoscopy cases when measured with the GAGES tool.
Surg Endosc. 2014 May;28(5):1494-9. doi: 10.1007/s00464-013-3339-z. Epub 2013 Dec 12.
Endoscopic simulator curriculum improves colonoscopy performance in novice surgical interns as demonstrated in a swine model.
Telem DA1, Rattner DW, Gee DW.
1Division of Laparoscopic, Bariatric and Advanced GI Surgery, Stony Brook University Medical Center, Stony Brook, NY, USA,
INTRODUCTION: The purpose of this study was to determine whether independent virtual endoscopic training accelerates the acquisition of endoscopic skill by novice surgical interns.
METHODS: Nine novice surgical interns participated in a prospective study comparing colonoscopy performance in a swine model before and after an independent simulator curriculum. An independent observer evaluated each intern for the ability to reach the cecum within 20 min and technical ability as determined by Global Assessment of Gastrointestinal Endoscopic Skills-Colonoscopy (GAGES-C) score and performance compared. In addition, at the conclusion of training, a post test of two basic simulated colonoscopy modules was completed and metrics evaluated. As a control, three attending physicians who routinely perform colonoscopy also completed colonoscopy in the swine model.
RESULTS: Prior to endoscopic training, one (11 %) intern successfully intubated the cecum in 19.56 min. Following training, six (67 %) interns reached the cecum with mean time of 9.2 min (p < 0.05). Statistically significant improvement was demonstrated in four out of five GAGES-C criteria. All three experts reached the cecum, with a mean time of 4.40 min. Comparison of expert and post-curriculum intern times demonstrated the experts to be significantly faster (p < 0.05). Comparison of interns who were and were not able to reach the cecum following the simulator curriculum demonstrated significantly improved GI Mentor™ performance in the efficiency (79 vs. 67.1 %, p = 0.05) and time to cecum (3.37 vs. 5.59 min, p = 0.01) metrics. No other significant difference was demonstrated in GAGES-C categories or other simulator parameter.
CONCLUSION: Simulator training on the GI Mentor™ alone significantly improved endoscopic skills in novice surgical interns as demonstrated in a swine model. This study also identified parameters on the GI Mentor™ that could indicate ‘clinical readiness’. This study supports the role for endoscopic simulator training in surgical resident education as an adjunct to clinical experience.
Why fundamentals of endoscopic surgery (FES)?
Hazey JW, Marks JM, Mellinger JD, Trus TL, Chand B, Delaney CP, Dunkin BJ, Fanelli RD, Fried GM, Martinez JM, Pearl JP, Poulose BK,Sillin LF, Vassiliou MC, Melvin WS.
Section of Minimally Invasive Surgery, Department of Surgery, The Wexner Medical Center, The Ohio State University, N708 Doan Hall, 410 West Tenth Avenue, Columbus, OH, 43210, USA,
Surg Endosc. 2013 Dec 7.
Fundamentals of endoscopic surgery: creation and validation of the hands-on test.
Vassiliou MC, Dunkin BJ, Fried GM, Mellinger JD, Trus T, Kaneva P, Lyons C, Korndorffer JR Jr, Ujiki M, Velanovich V, Kochman ML, Tsuda S, Martinez J, Scott DJ, Korus G, Park A, Marks JM.
Surg Endosc. 2013 Nov 20.
BACKGROUND: The Fundamentals of Endoscopic Surgery™ (FES) program consists of online materials and didactic and skills-based tests. All components were designed to measure the skills and knowledge required to perform safe flexible endoscopy. The purpose of this multicenter study was to evaluate the reliability and validity of the hands-on component of the FES examination, and to establish the pass score.
METHODS: Expert endoscopists identified the critical skill set required for flexible endoscopy. They were then modeled in a virtual reality simulator (GI Mentor™ II, Simbionix™ Ltd., Airport City, Israel) to create five tasks and metrics. Scores were designed to measure both speed and precision. Validity evidence was assessed by correlating performance with self-reported endoscopic experience (surgeons and gastroenterologists [GIs]). Internal consistency of each test task was assessed using Cronbach’s alpha. Test-retest reliability was determined by having the same participant perform the test a second time and comparing their scores. Passing scores were determined by a contrasting groups methodology and use of receiver operating characteristic curves.
RESULTS: A total of 160 participants (17 % GIs) performed the simulator test. Scores on the five tasks showed good internal consistency reliability and all had significant correlations with endoscopic experience. Total FES scores correlated 0.73, with participants’ level of endoscopic experience providing evidence of their validity, and their internal consistency reliability (Cronbach’s alpha) was 0.82. Test-retest reliability was assessed in 11 participants, and the intraclass correlation was 0.85. The passing score was determined and is estimated to have a sensitivity (true positive rate) of 0.81 and a 1-specificity (false positive rate) of 0.21.
CONCLUSIONS: The FES hands-on skills test examines the basic procedural components required to perform safe flexible endoscopy. It meets rigorous standards of reliability and validity required for high-stakes examinations, and, together with the knowledge component, may help contribute to the definition and determination of competence in endoscopy.
The following abstract was presented at Annual Digestive Disease Week (DDW), May 18-21, 2013, Orlando, Florida
Sequential Analysis of the Ergonomics of First Year Gastroenterology Fellows With Simulated Endoscopy to Assess Effect of Practice on Range of Motion: an Attempt to Reduce Musuloskeletal Injury During Endoscopy
Kevin C. Ruff1, Deepika Mohankumar2, Mary A. Atia1, Shiva K. Ratuapli1, Darren Andrade1, Michael Foley1, Bobby R. Kakati1, Marco Santello2, David E. Fleischer1, Francisco C. Ramirez1
Mayo Clinic, Scottsdale, Arizona, Arizona State University, Phoenix, Arizona
BACKGROUND: The relationship between musculo-skeletal injuries and endoscopy performance is not well understood. Studying the ergonomics and kinematics of the procedure may provide information about the cause of these injuries.
AIM: The aim of the study was to determine the effect of practice on the range of motion of the wrist joints during performance of simulated colonoscopy in first year Gastroenterology fellows prior to and after a period of formal endoscopic training.
MATERIALS AND METHODS: Five first year Gastroenterology fellows (4 men, 1 woman; all right-handed, one ambidextrous fellow) participated in the study. Simulations of colonoscopy were performed (GI Mentor Endoscopy), one practice and 2 experimental trials for each subject. The trials were up to 10 minutes in length with 1 easy and 1 difficult procedure as described by the simulator manual. Procedures were completed in counterbalanced order across subjects. Wrist kinematics were recorded in two sessions, one at the start of fellowship training (“baseline) and one three months later (“follow-up”).
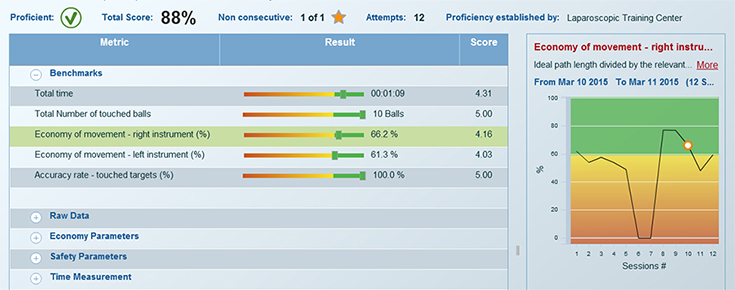
Right forearm kinematics were measured using a magnetic position/orientation tracker (Fastrak, Polhemus; 120 Hz sampling rate). We measured three degrees of freedom (DoF) of wrist motion: pronation/supination, flexion/extension, and abduction/adduction. We defined four different zones based on the wrist angle relative to the extreme and the center ranges of motion: center, mid, extreme, and out of range. (see Figure 1 for data of single procedure) The time spent in each of these zones was calculated and statistical analysis was performed to determine whether three months of endoscopy practice had any affect.
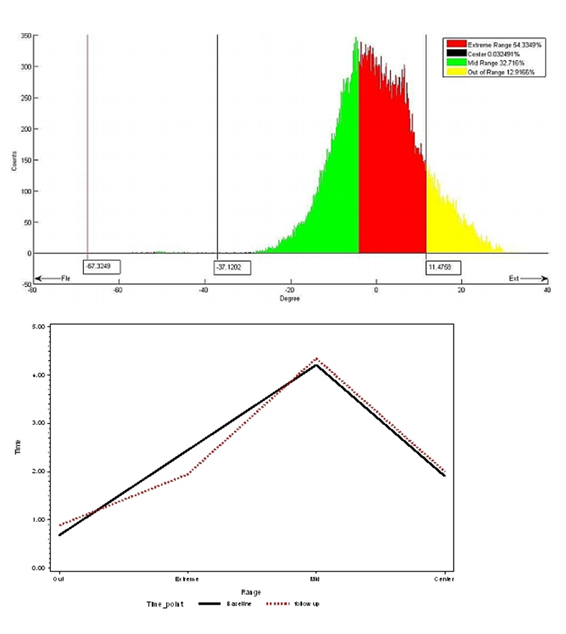
RESULTS: Fellows performed an average of 150 endoscopic procedures in between the two measurement periods. Mixed model analysis of the time spent in each wrist movement zone revealed that three months of endoscopy practice did not significantly change the time spent in each zone for any degree of freedom. Fellows spent most time in the mid range followed by the extreme range at both baseline and follow-up sessions (p <0.0001). (see Figure 2)
CONCLUSIONS: Although our pilot study was conducted on a small number of subjects, our data indicate that tracking wrist motion and time spent at extreme ranges of motions during endoscopy training is a promising approach that may lead to improving training procedures and potentially minimize the risk of musculoskeletal injuries. The fact that the time spent in each movement zone did not change after three months suggests that training (practice) led subjects to use the same movement patterns used in the baseline session while executing the endoscopic maneuvers. This continuous, ongoing sequential analysis will allow us to observe patterns in a cohort of Gastroenterology fellows beginning at the start of their endoscopic training.
Disclosure: Kevin C. Ruff – Consulting: ProVation
David E. Fleischer – Grant/Research Support: BARRX Medical, Fujinon, Olympus America
The following people have nothing to disclose: Deepika Mohankumar, Mary A. Atia, Shiva K. Ratuapli, Darren Andrade, Michael Foley, Bobby R. Kakati, Marco Santello, Francisco C. Ramirez
Все тезисы можно посмотреть здесь
- Воронежский государственный медицинский университет
- Московский государственный медико-стоматологический университет им.А.И. Евдокимова
- НМИЦ здоровья детей
- Российский университет дружбы народов
- Рязанский государственный медицинский университет
- Тюменский государственный медицинский университет
- Ярославский государственный медицинский университет
