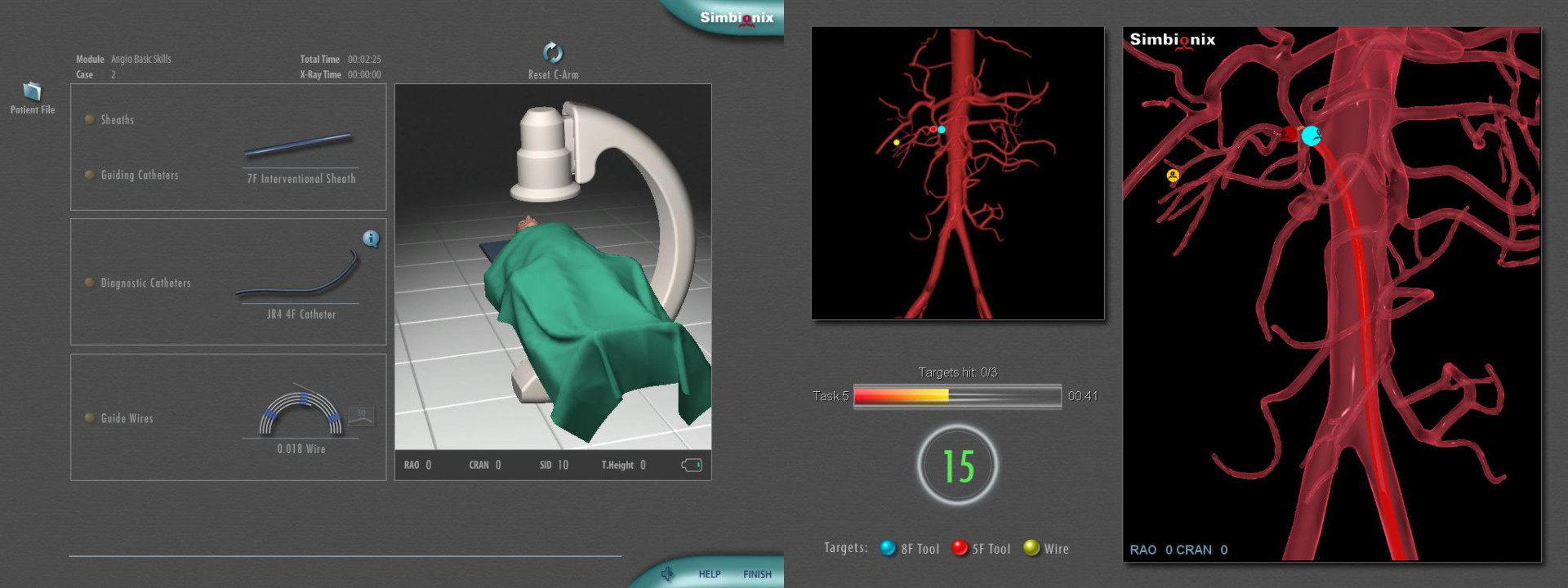
АнгиоМентор - симулятор рентгенэндоваскулярных вмешательств
.jpg)





































-koronarnyix-arterij.jpg)
.png)
















-koronarnyix-arterij.jpg)
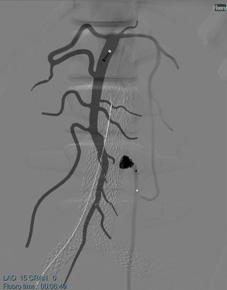
Вмешательства на сосудах под контролем рентгеноскопии отличаются не только сложностью и точностью выполнения манипуляций, но и облучением как пациента, так и членов операционной бригады. Повышению радиационной безопасности, снижению лучевой нагрузки и времени операции, сокращению использования контраста способствует регулярное обучение в безопасных условиях с использованием симуляционного оборудования.
АнгиоМентор – это уникальный симулятор для обучения более 30 типам рентгенэндоваскулярных вмешательств.
Более 230 клинических случаев отражают не только все многообразие существующих патологий, но и вариантную анатомию различных пациентов.
С симулятором АнгиоМентор вы не ограничены узким набором клинических случаев: благодаря опции iCase вы сможете самостоятельно создавать и редактировать неограниченное их количество.
АнгиоМентор – не просто отдельный симулятор для отработки конкретного навыка, а целая виртуальная гибридная операционная в Вашем симуляционном центре. Это возможно благодаря опции интеграции настоящей С-дуги.
Параллельно с освоением технических навыков симулятор АнгиоМентор позволяет проводить командный тренинг для улучшения коммуникативных навыков, оптимизации взаимодействия членов хирургической бригады, процесса принятия решений как в плановых, так и в экстренных ситуациях.
Симулятор используется для обучения врачей по всему миру. Только в Европе на сегодняшний день уже установлено около 280 АнгиоМенторов, список пользователей симулятора в нашей стране также непрерывно пополняется (см. вкладку Наши клиенты).
АнгиоМентор находит также применение в клинической практике. Уникальное программное обеспечение Procedure Rehearsal Studio позволяет загрузить данные КТ пациента и отрепетировать операцию на симуляторе, что поможет избежать возможных осложнений, сократить время операции, заранее подобрать нужные инструменты.
Характеристики
- 5 точек доступа:
- бедренный с двух сторон
- подключичный
- доступ на стопе
- доступ на лучевой артерии
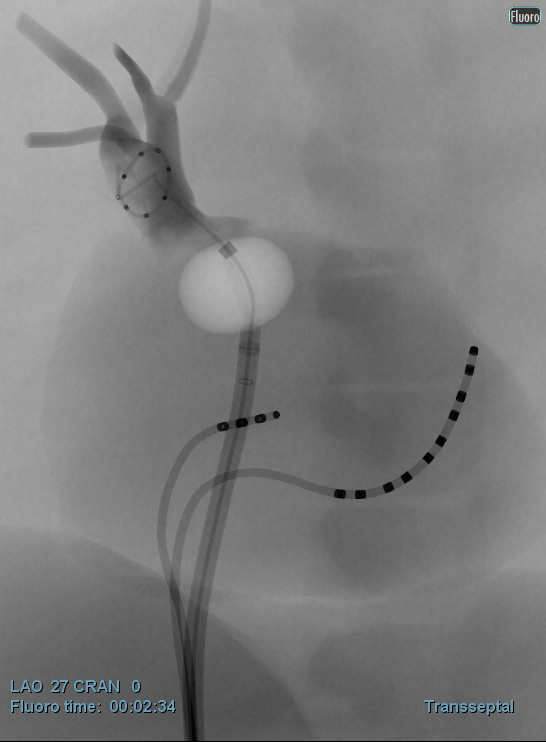
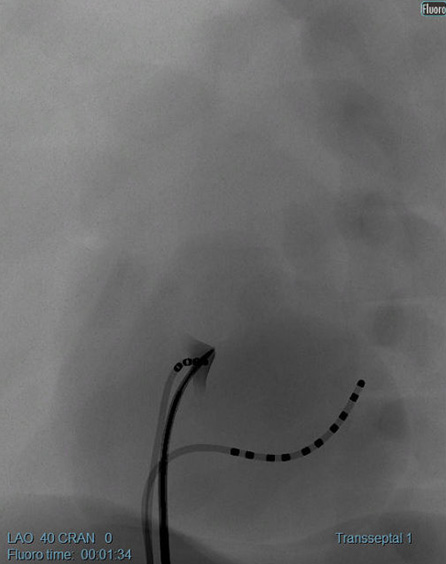
- Симуляция эндоваскулярных процедур с одновременным доступом с двух сторон, что необходимо для операций EVAR/TEVAR (правая и левая бедренные артерии), пункция межпредсердной перегородки (бедренная вена и артерия).
- Обратная тактильная связь с реалистичными ощущениями, как во время настоящей операции, использование до 6 инструментов одновременно.
- 2 экрана:
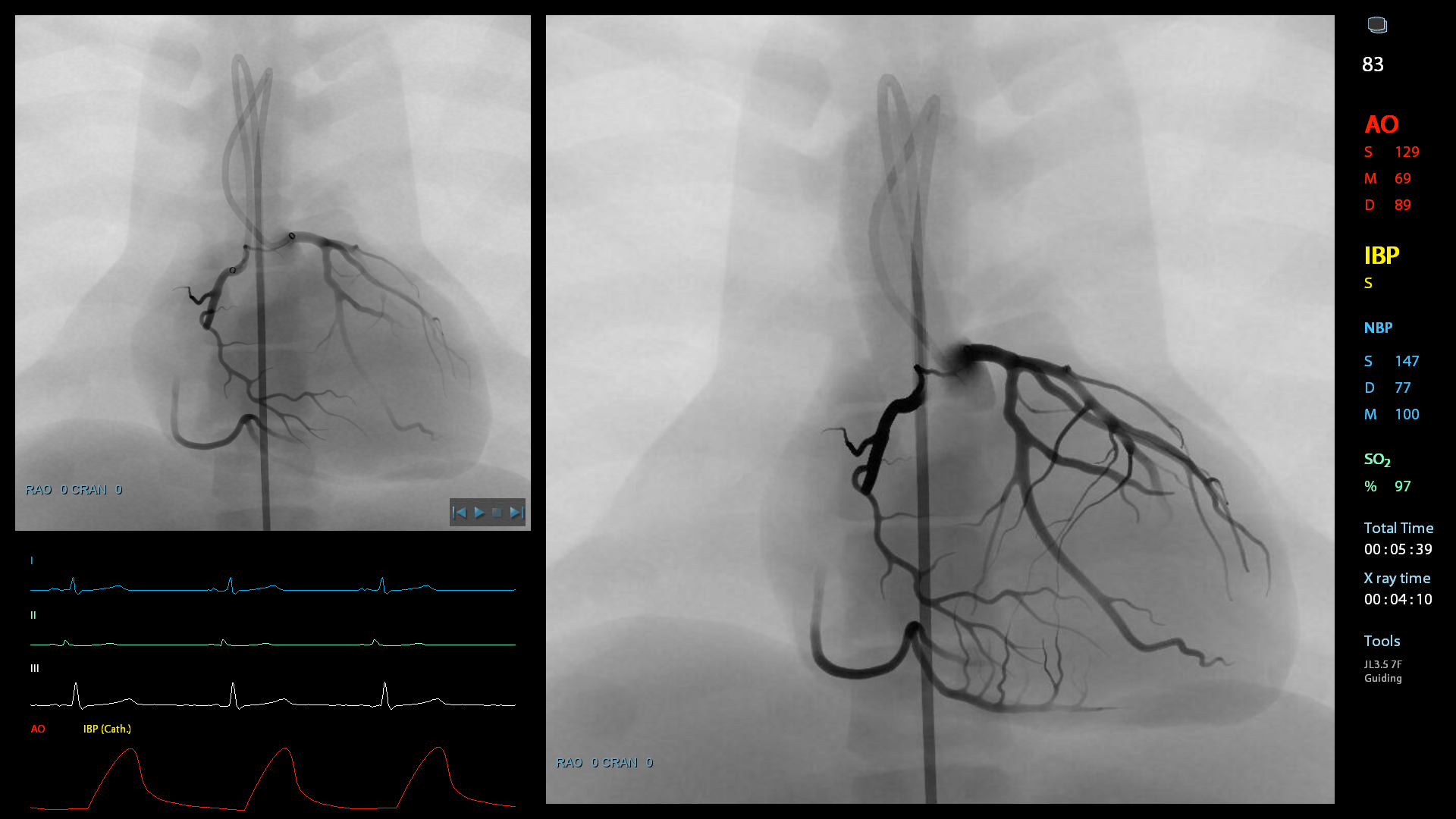
- Экран 49" для флюороскопии, 3D и визуализации монитора пациента.
- Панель 19" с сенсорным экраном для управления ходом симуляции (выбор инструментов, лекарственных препаратов, контроль инструментов)
- Манекен пациента, накрытый хирургической простынью
- Регулируемый по высоте и расширяемый операционный стол
- Встроенная панель для управления виртуальной С-дугой и столом
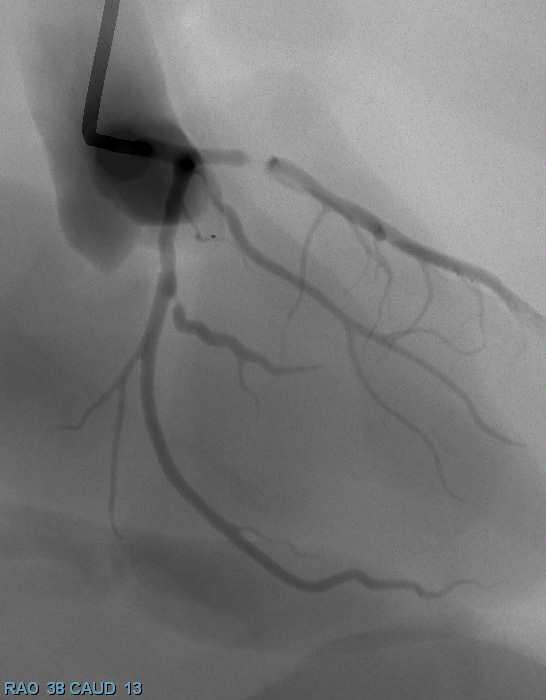
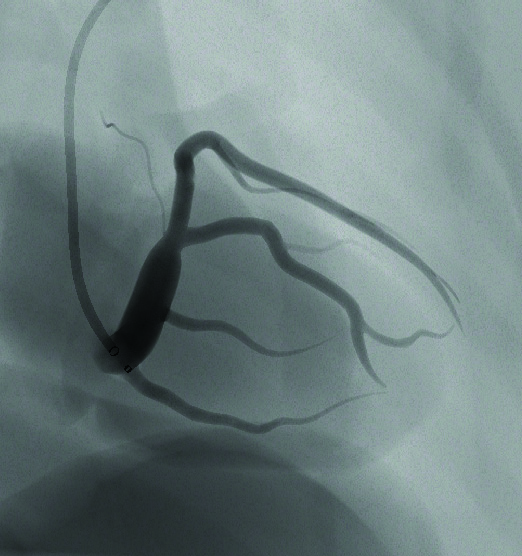
- Рентгеноскопическое изображение меняется в точном соответствии с положением виртуальной С-дуги, что дает возможность обучиться навыкам позиционирования и получения необходимой проекции
- Базовые инструменты: проводниковый катетер 8F, диагностический катетер 5F, проводник 0.035", проводник 0.014", катетер быстрого обмена, шприц для введения контраста, инструмент для раскрытия стента, устройство раздувающее баллон. Дополнительные инструменты зависят от выбранного модуля.
- Педальный блок с 3 педалями для флюороскопии
- Большой ящик для хранения инструментов
- Датчик ТЕЕ при работе с модулем транспищеводной эхокардиографии
- Мониторинг показателей жизнедеятельности виртуального пациента
- Индикаторы дозы облучения
- Обширная библиотека виртуальных инструментов
Обучающий контент
- задания с интерактивным контролем с различными уровнями сложности позволяют осваивать навыки от базовых до продвинутых
- пошаговые инструкции по выполнению процедуры с интерактивными подсказками
- сложные клинические сценарии с имитацией осложнений и повреждений в режиме реального времени дают возможность приобретать опыт различных подходов к выполнению процедуры
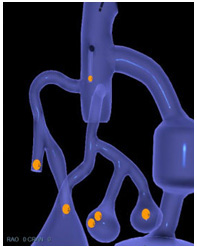
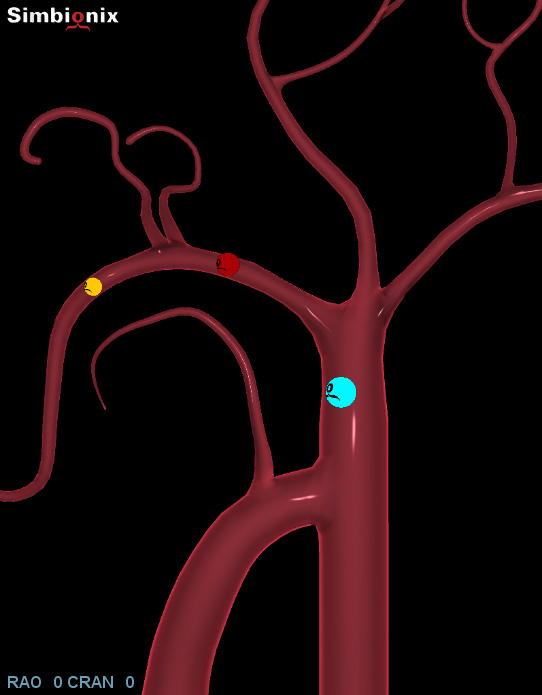
- подробная анатомия, трехмерная визуализация операционного стола и С-дуги облегчают понимание
- дидактические материалы включают видео-записи реальных операций
- симулятор валидирован в исследованиях по всему миру в течение последних 6 лет
- постоянно разрабатываемые новые модули в соответствии с динамично развивающимися медицинскими технологиями
МенторЛерн
Уникальная система управления учебным процессом на всех симуляторах Simbionix
Подробнее про МенторЛерн
Варианты комплектации
|
SXANSUB |
Симулятор АнгиоМентор + 4 базовых модуля |
|
SXANSUB3 |
Симулятор АнгиоМентор + 4 базовых модуля + 3 модуля на выбор |
|
SXANSU6 |
Симулятор АнгиоМентор + 4 базовых модуля + 6 модулей на выбор |
|
SXANSU10 |
Симулятор АнгиоМентор + 4 базовых модуля + 10 модулей на выбор |
|
SXANSU15-IC |
Симулятор АнгиоМентор + 4 базовых модуля + 15 модулей на выбор + конструктор кейсов iCase |
|
SXANSUF-IC |
Симулятор АнгиоМентор со всеми доступными модулями + конструктор кейсов iCase |
Опции С-дуги
SXAN-MINICA Модель мини С-дуги для обучения базовым навыкам управления
|
SXANCC |
Интеграция С-дуги, имеющейся у заказчика, с симулятором АнгиоМентор |
|
SXANCS |
Имитатор ручной С-дуги, интегрированный с симулятором АнгиоМентор |
Чреспищеводная ЭхоКГ
|
SXAN-TEEI |
Пакет дополнений "Чреспищеводная эхокардиография" для симулятора АнгиоМентор Включает имитатор чреспищеводного УЗ-датчика, подставку для датчика, модуль "TEE - чреспищеводная эхокардиография" + 1 модуль на выбор из категории модулей, совместимых с опцией "ЧПЭхоКГ" |
SX-PWPU Годовое постгарантийное обслуживание симулятора
Базовые модули
- Базовые навыки эндоваскулярных вмешательств
- Базовые навыки в электрофизиологии
- Базовые навыки в кардиологии
- Основы работы с С-дугой
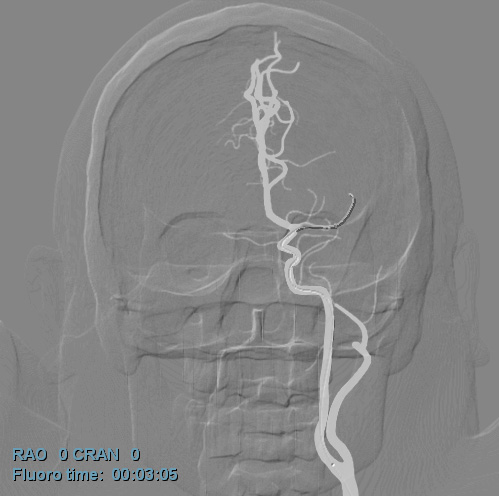
Нейроваскулярные вмешательства
- Вмешательства на сонных артериях
- Вмешательства на сосудах головного мозга
- Острый ишемический инсульт
- Вмешательства но сосудах головного мозга через трансрадиальный доступ
Вмешательства на сосудах сердца
- Вмешательства на коронарных артериях
- Бифуркация коронарных артерий
- ХТО коронарных артерий
- Трансрадиарные вмешательства на коронарных артериях
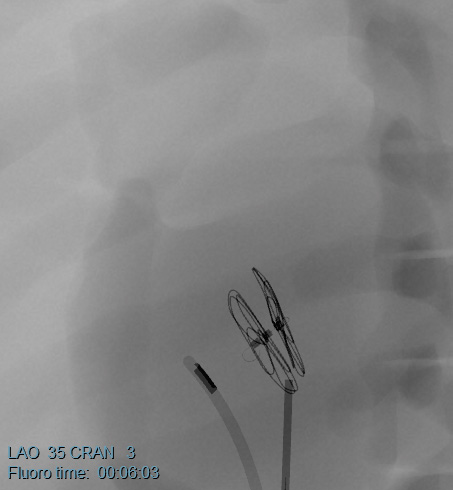
Структурные заболевания сердца
- Протезирование аортального клапана
- Окклюзия дефекта межпредсердной перегородки открытого овального окна с опцией ЧПЭхоКГ
- Окклюзия ушка левого предсердия
Электрофизиология
- Управление сердечным ритмом
- Пункция межпредсердной перегородки с опцией ЧПЭхоКГ
- Аблация при фибрилляции предсердий
- Электрофизиологическое картирование сердца
- Внутрисердечная ЭхоКГ
Эмболизация
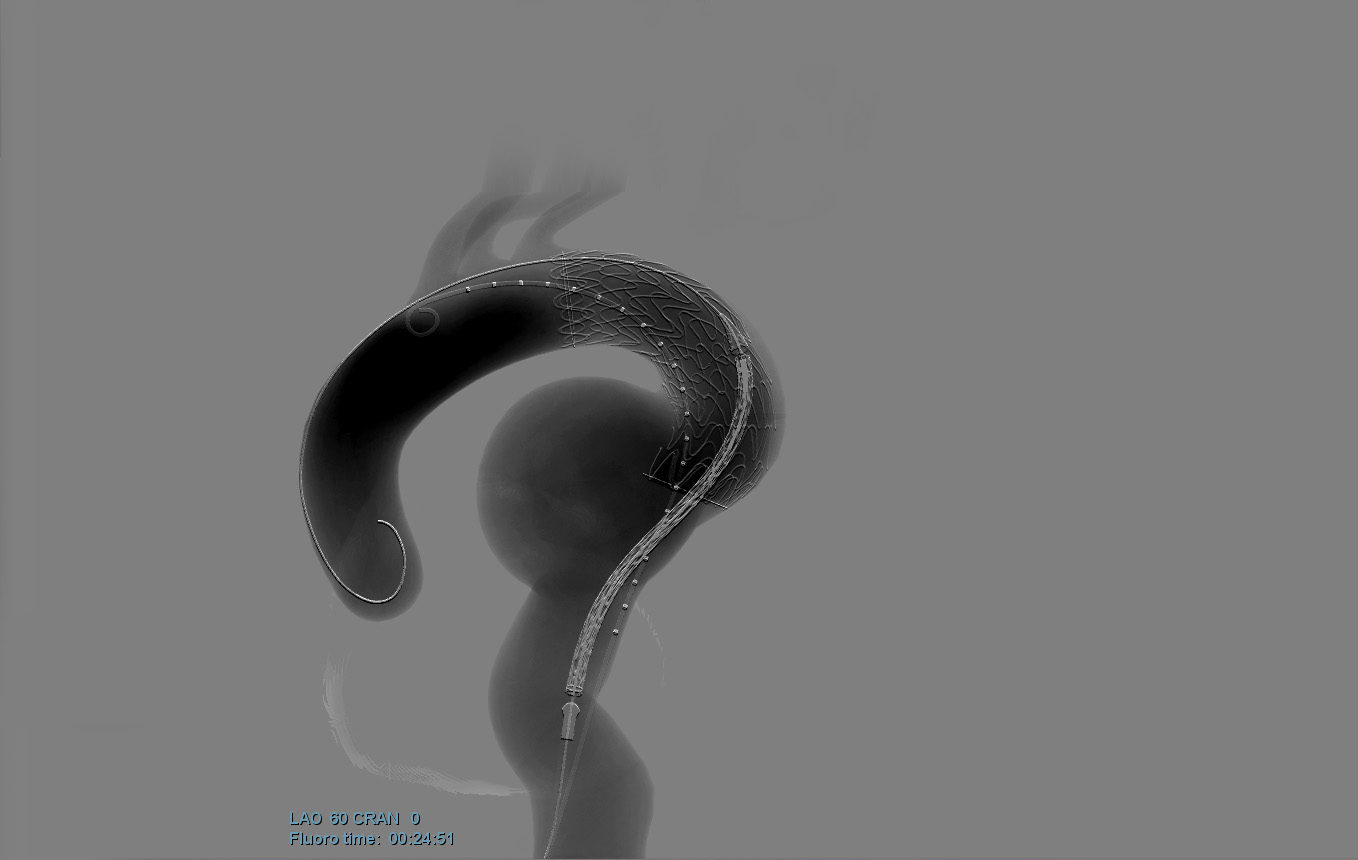
Вмешательства на аорте
- Эндоваскулярная реконструкция аневризмы брюшной аорты EVAR
- Эндоваскулярная реконструкция аневризмы грудной аорты TEVAR
- Расширенная эндоваскулярная реконструкция аневризмы грудной аорты TEVAR
Вмешательства на периферических сосудах
- Вмешательства на почечных артериях
- Вмешательства на подвздошных артериях, поверхностной бедренной артерии и сосудах ниже колена
- ХТО артерий нижних конечностей
- Атерэктомия
- Венозные вмешательства
- Тромбэктомия при ТЭЛА (НОВИНКА)
- Венозные вмешательства на подвздошно-бедренных сосудах — скоро
Экстренные вмешательства
The Role of Simulation in Boosting the Learning Curve in EVAR Procedures
Vento V, Cercenelli L, Mascoli C., Gallitto E., Ancetti S., Faggioli G., Freyrie A., Marcelli E., Gargiulo M., Stella A.
OBJECTIVE: Simulation may be a useful tool for training in endovascular procedures. The aim of this study was to evaluate the effect of endovascular repair of abdominal aortic aneurysms (EVAR) simulation in boosting trainees’ learning curve.
DESIGN: Ten vascular surgery residents were recruited and divided in 2 groups (Trainee Group and Control group). At a first session (t0), each resident performed 2 simulated EVAR procedures using an endovascular simulator. After 2 weeks, each participant simulated other 2 EVAR procedures in a final session (t1). In the period between t0 and t1, each resident in the Trainee Group performed 6 simulated EVAR procedures, whereas the Control Group did not perform any other simulation. Both quantitative and qualitative performance evaluations were performed at t0 and t1. Quantitative evaluation from simulator metrics included total procedural time (TP), total fluoroscopy time (TF), time for contralateral gate cannulation (TG), and contrast medium volume (CM) injected. Qualitative evaluation was based on a Likert scale used to calculate a total performance score referred to skills involving major EVAR procedural steps.
RESULTS: All residents in the Trainee Group significantly reduced TP (48 ± 12 vs 32 ± 8 minutes, t0 vs t1, p < 0.05), TF (18 ± 7 vs 11 ± 6 minutes, p < 0.05), and CM used over time (121 ± 37 vs 85 ± 26ml, p < 0.05), but not TG (5 ± 5 vs 3 ± 4 minutes, p = 0.284). In the Control Group metrics did not change significantly in any field (TP = 55 ± 11 vs 46 ± 10 minutes; TF = 25 ± 9 vs 21 ± 4 minutes; CM = 132 ± 51 vs 102 ± 42ml; TG = 6 ± 4 vs 8 ± 5 minutes, all p > 0.05). The average Trainee Group qualitative total performance score improved significantly (p < 0.05) after rehearsal sessions when compared with the Control Group. CONCLUSION:Simulation is an effective method to improve competence of vascular surgery residents with EVAR procedures.
Copyright © 2018 Association of Program Directors in Surgery. Published by Elsevier Inc. All rights reserved.
Endovascular Training Using a Simulation Based Curriculum is Less Expensive than Training in the Hybrid Angiosuite
Maertens H., Vermassen F., Aggarwal R., Doyen B., Desender L., Van Herzeele I., Annemans L.
Eur J Vasc Endovasc Surg (2018) 56, 583-590
OBJECTIVE/BACKGROUND: This study aimed to determine the cost-effectiveness of a PROficiency based StePwise Endovascular Curricular Training (PROSPECT) program, including e-learning and hands on virtual reality simulation.
METHODS: A prospective, single blinded, randomised controlled trial (RCT) was carried out to evaluate the impact of a PROSPECT training program on real life operative performance. Under supervision, all subjects performed two endovascular interventions on patients with symptomatic iliac and/or superficial femoral artery stenosis. Primary outcomes were technical performance (Global Rating Scale, Examiner Checklist), operative metrics, and patient outcomes, adjusted for case difficulty and the trainee’s experience. Additionally, an analysis of costs and savings related to implementation of this endovascular training program was performed. Thirty-two general surgery trainees were randomised into three groups: group 1 (n = 11) received e-learning and simulation training (PROSPECT program); group 2 (n = 10) only had access to e-learning; group 3 (n = 11) did not receive supplementary education besides clinical training. Developmental cost, implementation cost, training time cost, and the operational cost of PROSPECT were determined. Time spent studying and practicing was converted to indirect saving of operating time. The costs of logistics, faculty time supervising simulation sessions, and 30 day complication rates were registered. Sensitivity analysis was performed to assess the robustness of the results.
RESULTS: Fifty-eight peripheral endovascular interventions, performed by 29 surgical trainees (three dropouts) were included in this RCT from October 2014 to February 2016. Annual costs from the perspective of the hospital were €6589 for curriculum design, €31,484 for implementation, and €1143 in operational costs. Per trainee, simulation based training until proficiency cost €3806. In comparison, if endovascular proficiency levels were obtained with conventional training only, this may have cost €5001 per trainee.
CONCLUSION: Simulation based training in endovascular procedures may be cost saving, because training occurs outside the angiosuite. It is possible that cost savings are underestimated as, in contrast to the literature, prevented costs related to complications could not be defined.
Role of Simulation in Endovascular Aneurysm Repair (EVAR) Training: A Preliminary Study
Saratzis A, Calderbank T, Sidloff D, Bown MJ, Davies RS.
BACKGROUND: Endovascular aneurysm repair (EVAR) requires a high-level of technical-competency to avoid device-related complications. Virtual reality simulation-based training (SBT) may offer an alternative method of psychomotor skill acquisition; however, its role in EVAR training is undefined. This study aimed to: a) benchmark competency levels using EVAR SBT, and b) investigate the impact of supervised SBT on trainee performance.
METHODS: EVAR procedure-related metrics were benchmarked by six experienced consultants using a Simbionix Angiomentor EVAR simulator. Sixteen vascular surgical trainees performing a comparable EVAR before and after structured SBT (>4 teaching sessions) were assessed utilising a modified Likert-scale score. These were benchmarked for comparison against the standard set by the consultant body.
RESULTS: Median procedural-time for consultants was 43.5 min (IQR 7.5). A significant improvement in trainee procedural-time following SBT was observed (median procedural time 77 min [IQR 20.75] vs. 56 min [IQR: 7.00], p < .0001). The mean (SD) trainee Likert score pre- and post-SBT improved (16.6 [SD 1.455] vs. 28.63 [SD 2.986], p < .0001). Fewer endoleaks were observed (p = .0063) and trainees chose an appropriately sized device more often after SBT.
CONCLUSION: This study suggests that EVAR-SBT should be considered as an adjunct to standard psychomotor skill teaching techniques for EVAR within the vascular surgery training curricula.
Initial Results of an Original Program of Simulation Training for Endovascular Procedures
Georg ., Chenesseau B., Girsowicz E, Lejay A., Thaveau F., Papillon J., Lee J., Chakfe N.
USP, CHU de Strasbourg, Strasbourg, France
Ann Vasc Surg. 2017 Jan;38:e8-e9.
OBJECTIVES: The practice of simulation is currently swiftly developing. It makes it possible for students to carry out procedures in a controlled environ-ment without compromising the safety of patients. Endovascular surgery (EV) is ideal for practice on simulators and many models are currently available. We evaluated the first results of our program in a group of six residents beginning their training in vascular surgery.
MATERIALS AND METHODS: Our EV simulation program results from a collaborative project with Stanford University (California, USA) which is based on an evaluation of the various sequences composing an EV procedure according to a grid of evaluation comprising approximately 40 items. The procedures are carried out in a realistic environment reproducing a surgical unit. The simulator used was the ANGIO Mentor Suite (Simbionix) equipped with various modules (iliac, superficial femoral, EVAR). Each procedure was filmed using several cameras in order to evaluate the posture and the gestural of the trainees. After each procedure a “debriefing” was carried out so as to reconsider the sequences having generated difficulties and to reinforce the teaching impact. Each resident could take part in eight 2 hours sessions and was evaluated on procedures of increasing difficulty adapted to his skills. The procedures included diagnostic angiography (DA), iliac angioplasty (IA) and superficial femoral (SFA) angioplasty by crossover. At the end of each session, the residents evaluated the teaching content using a questionnaire.
RESULTS: Six residents took part in the program. None of them had preliminary experience in EV surgery. The rate of participation in the sessions was 77% (62-100%). The average progression on a scale from 0 to 100 was 24 (9-46) for DA, 35 (30-42) for IA and 21 (5-42) for the SFA. The global evaluation of the sessions by the residents showed an average score of 4.6/5.
CONCLUSION: The regular practice of simulation according to a standardized and evaluated program improves the performance of the residents on EV procedures. The feeling of the residents was excellent and they were eager to be able to take advantages of simulation sessions. EV training by simulation has a place to train the residents in vascular surgery.
A Proficiency Based Stepwise Endovascular Curricular Training (PROSPECT) Program Enhances Operative Performance in Real Life: A Randomised Controlled Trial
This study was presented at the prize session at the European Society for Vascular Surgery annual meeting, Copenhagen, September 28–30, 2016.
Eur J Vasc Endovasc Surg (2017) 54, 387-396
Maertens a,* , R. Aggarwalb,c , N. Moreels a , F. Vermassen a , I. Van Herzeele a
a Department of Thoracic and Vascular Surgery, Ghent University Hospital, Ghent, Belgium
b Department of Surgery, Faculty of Medicine, McGill University, Montreal, Canada
c Steinberg Centre for Simulation and Interactive Learning, Faculty of Medicine, McGill University, Montreal, Canada
OBJECTIVES: Healthcare evolution requires optimisation of surgical training to provide safe patient care. Operating room performance after completion of proficiency based training in vascular surgery has not been investigated.
DESIGN: A randomised controlled trial evaluated the impact of a Proficiency based Stepwise Endovascular Curricular Training program (PROSPECT) on the acquisition of endovascular skills and the transferability of these skills to real life interventions. Materials: All subjects performed two endovascular interventions treating patients with symptomatic iliac and/or superficial femoral artery stenosis under supervision. Primary outcomes were technical performances (Global Rating Scale [GRS]; Examiner Checklist), operative metrics, and patient outcomes, adjusted for case difficulty and trainee experience. Secondary outcomes included knowledge and technical performance after 6 weeks and 3 months.
METHODS: Thirty-two general surgical trainees were randomised into three groups. Besides traditional training, the first group (n ¼ 11) received e-learning and simulation training (PROSPECT), the second group (n ¼ 10) only had access to e-learning, while controls (n ¼ 11) did not receive supplementary training.
RESULTS: Twenty-nine trainees (3 dropouts) performed 58 procedures. Trainees who completed PROSPECT showed superior technical performance (GRS 39.36 2.05; Checklist 63.51 3.18) in real life with significantly fewer supervisor takeovers compared with trainees receiving e-learning alone (GRS 28.42 2.15; p ¼ .001; Checklist 53.63 3.34; p ¼ .027) or traditional education (GRS 23.09 2.18; p ¼ .001; Checklist 38.72 3.38; p ¼ .001). Supervisors felt more confident in allowing PROSPECT trained physicians to perform basic (p ¼ .006) and complex (p ¼ .003) procedures. No differences were detected in procedural parameters (such as fluoroscopy time, DAP, procedure time, etc.) or complications. Proficiency levels were maintained up to 3 months.
CONCLUSIONS: A structured, stepwise, proficiency based endovascular curriculum including e-learning and simulation based training should be integrated early into training programs to enhance trainee performance.
- Казанский государственный медицинский университет
- Национальный медицинский исследовательский центр нейрохирургии им. академика Н.Н. Бурденко
- Национальный медицинский исследовательский центр сердечно-сосудистой хирургии имени А. Н. Бакулева
- Первый Московский государственный медицинский университет имени И.М. Сеченова
- Ростовский государственный медицинский университет
- Рязанский государственный медицинский университет
- Смоленский государственный медицинский университет
