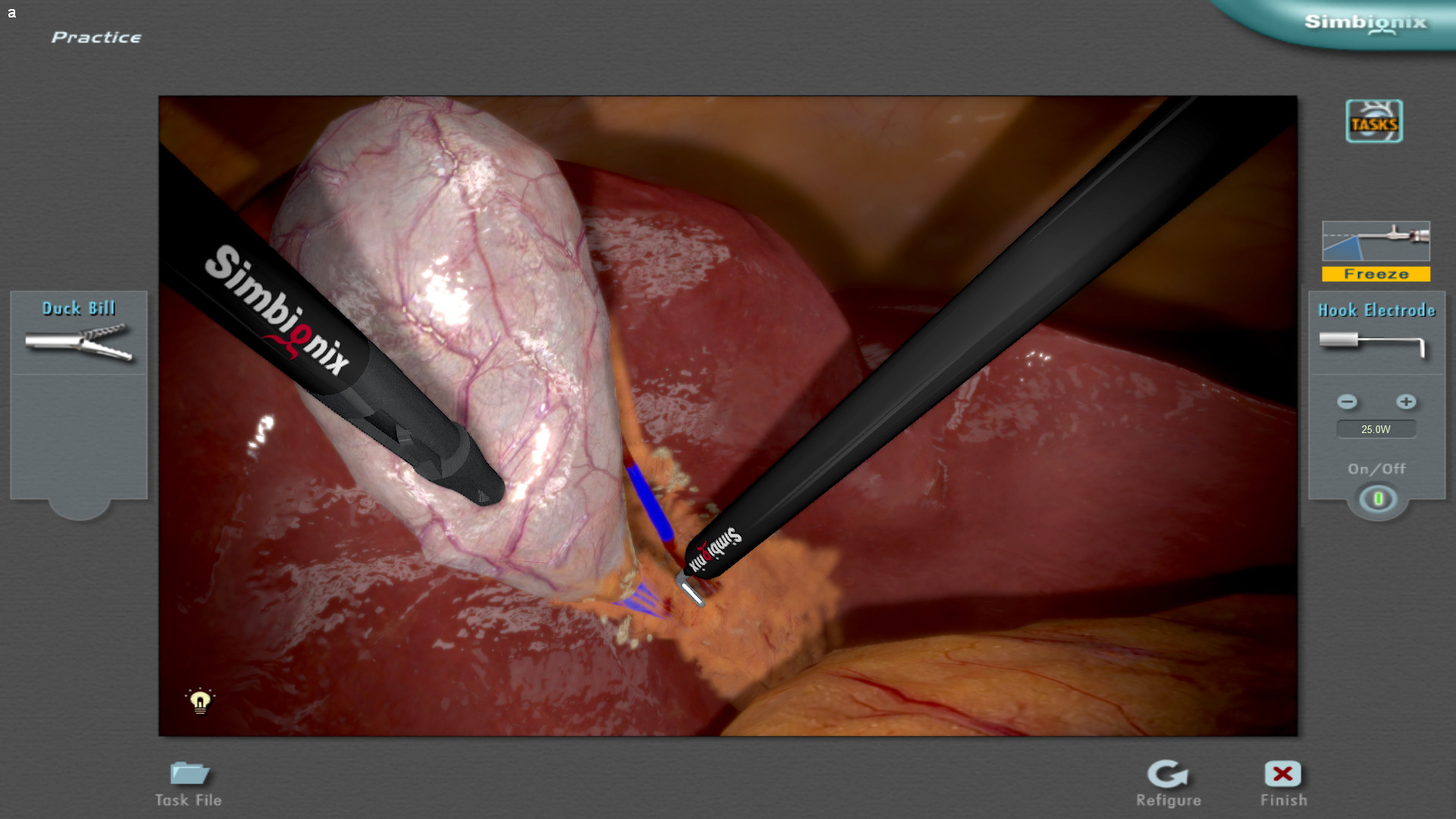
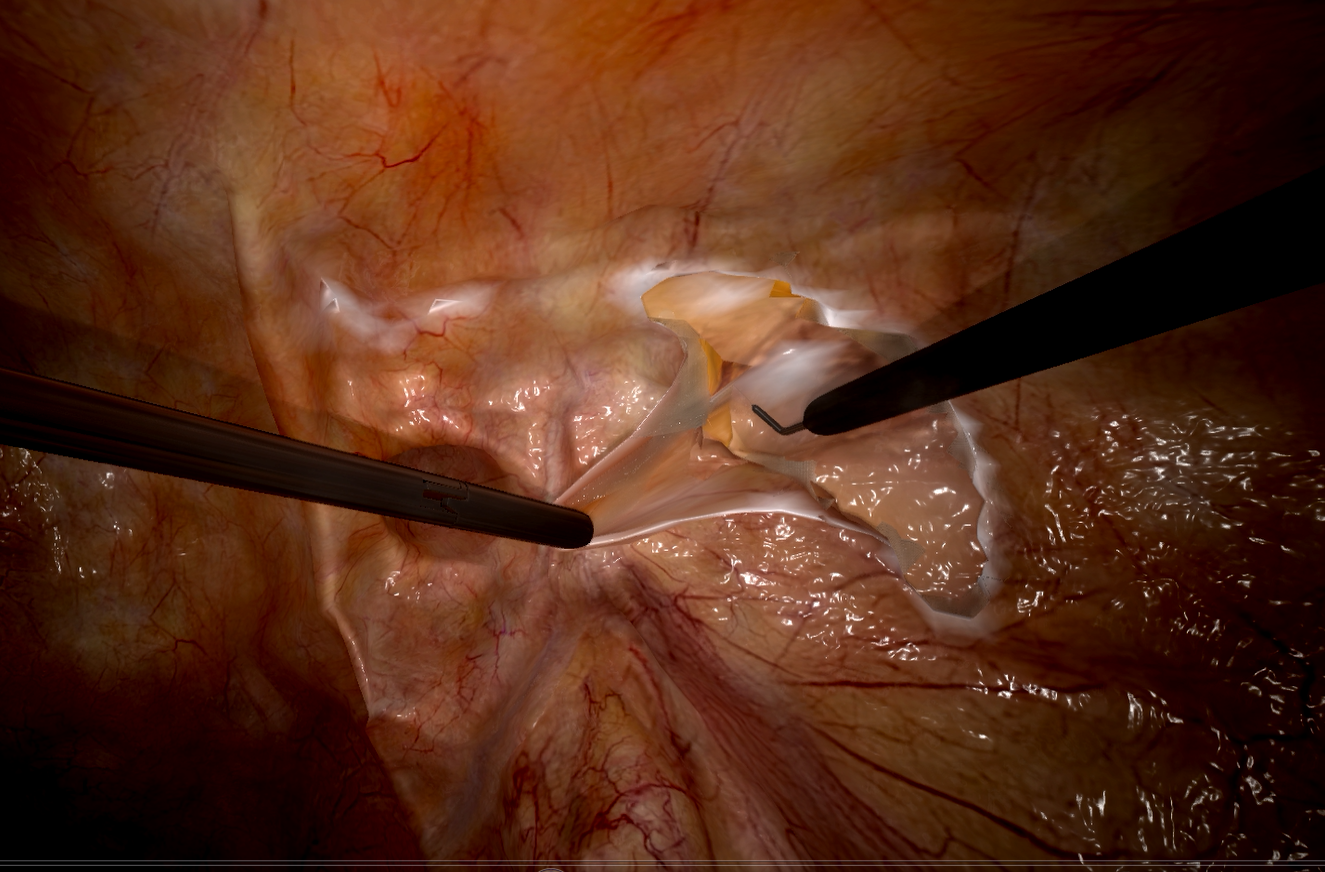
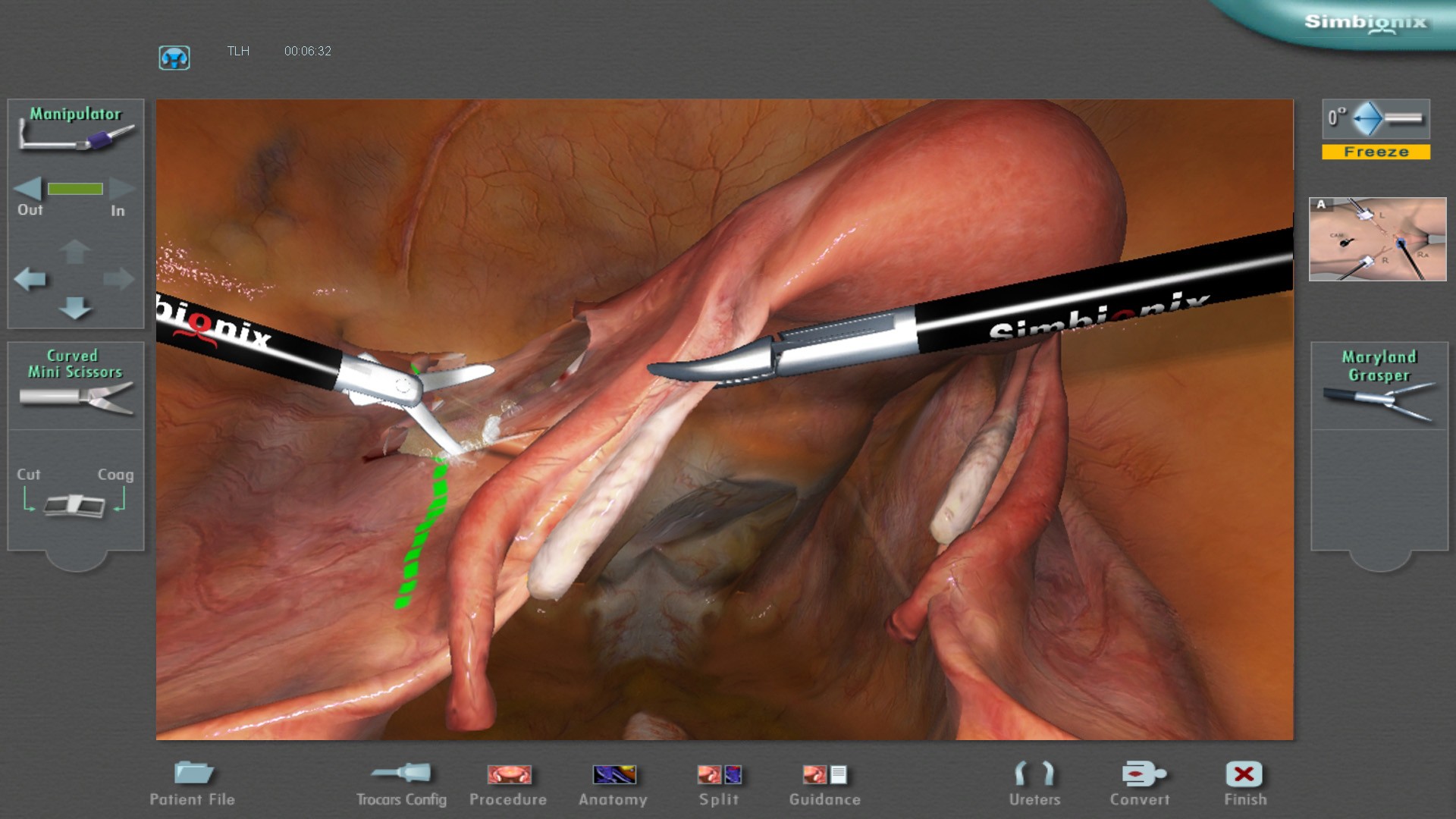
ЛапМентор - лапароскопический симулятор с обратной тактильной связью





































Современный симулятор, предлагающий 17 обучающих модулей и более 70 практических заданий по таким специальностям как:
- Хирургия
- Торакальная хирургия
- Колопроктология
- Бариатрическая хирургия
- Гинекология
- Урология
ЛапМентор содержит уникальные для данного типа симуляторов модули, посвященные обучению технике выполнения интраоперационной холангиографии и пластики послеоперационной вентральной грыжи из лапароскопического доступа.
НОВИНКА!!!
Усовершенствованная камера с расширенным функционалом

Характеристики
- Подвижная платформа на колесах с возможностью регулировки по высоте
- Сенсорный экран 24 дюйма
- Имитаторы лапароскопических инструментов с 5 степенями свободы
- Съемные рукоятки лапароскопических инструментов
- Имитатор камеры с 4 степенями свободы и выбором угла обзора 0º, 30º и 45º
- Непревзойденная точность отслеживания движений инструментов
- Реалистичная обратная тактильная связь
Обучающий контент
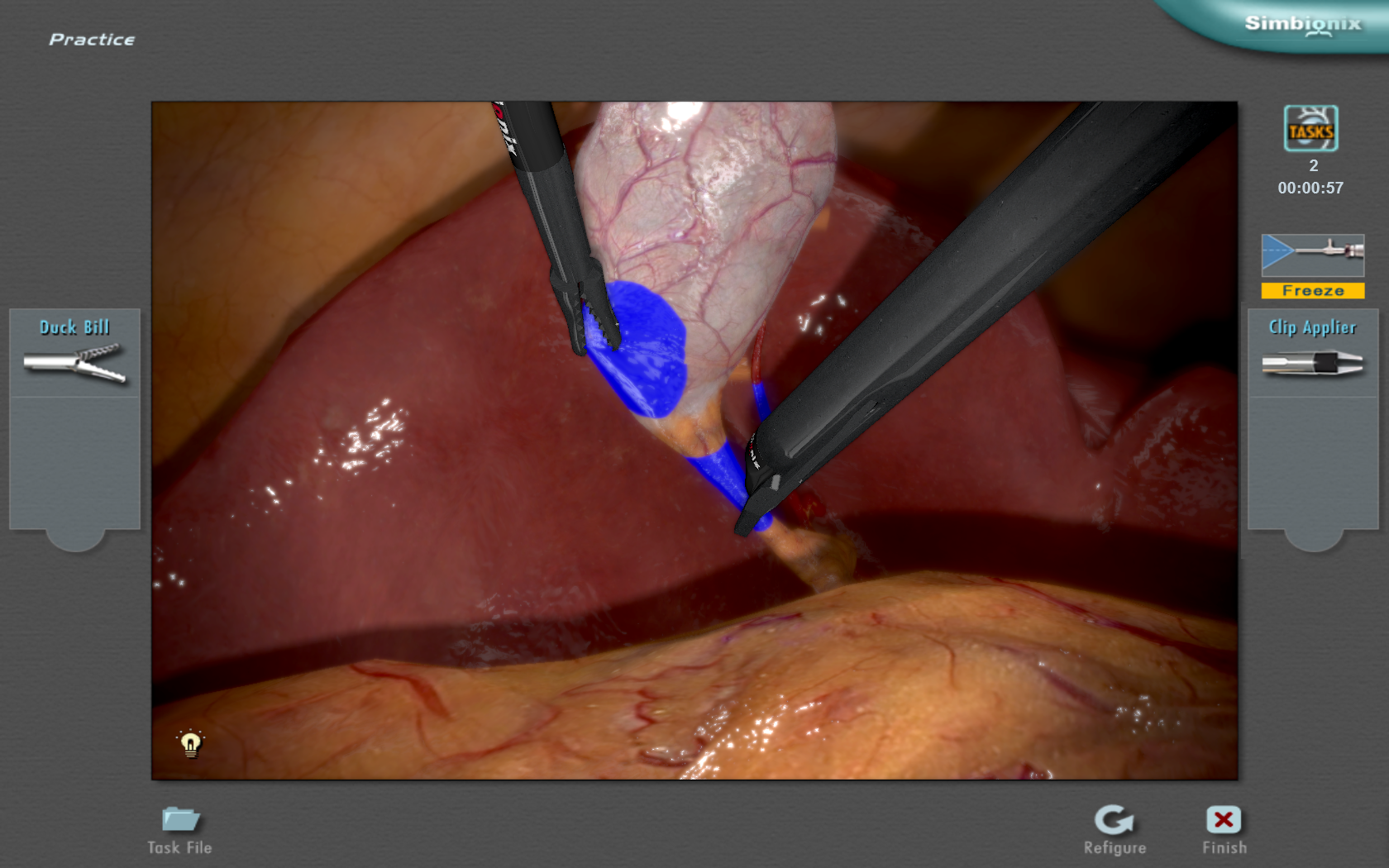
- задания с интерактивным контролем с различными уровнями сложности позволяют осваивать навыки в области лапароскопии от базовых до продвинутых
- сложные клинические сценарии с имитацией осложнений и повреждений в режиме реального времени дают возможность приобретать опыт различных подходов к выполнению процедуры
- комбинация реалистичной тактильной обратной связи, подробной анатомии, реалистичной визуализации, широкого диапазона хирургических инструментов и разнообразных конфигураций положения троакаров
- обучающий контент
- симулятор валидирован в более чем 60 исследованиях по всему миру
- дидактические материалы включают анатомические 3D-модели, поэтапные видео-записи реальных операций, интерактивные инструкции и готовые обучающие курсы
- всесторонние объективные отчеты и инструменты настройки уровня подготовленности для эффективного отслеживания прогресса в процессе обучения
- постоянно разрабатываемые новые модули в соответствии с динамично развивающимися медицинскими технологиями
На сегодняшний день уже установлено около 1330 ЛапМенторов по всему миру, и список пользователей симулятора в нашей стране постоянно пополняется (см. вкладку Наши клиенты).
МенторЛерн
Уникальная система управления учебным процессом на всех симуляторах Simbionix

Подробнее про МенторЛерн
Командный тренинг
Опция командного тренинга возможна при подключении портативного симулятора ЛапМентор Экспресс к ЛапМентор III, что позволяет осваивать навыки ассистента, тренировать нетехнические навыки и проводить тренировку в команде.
Режим Проктора и Выбора операционного инструментария

Режим Проктора даёт возможность наставнику вмешиваться в процесс отработки хирургической манипуляции в режиме реального времени, изменяя характеристики тканей в зависимости от уровня сложности, имитируя новые повреждения и кровотечения, ограничивая выбор инструментов, тем самым имитируя их выход из строя. Эта новая возможность позволит со стороны оценить способность тренируемого реагировать и принимать решения в неотложных ситуациях, качества, которые до этого не поддавались оценке в рутинной тренировке.
Режим выбора операционного инструментария позволяет помощнику (операционной сестре) менять инструментарий в ходе выполнения каждого конкретного задания, тем самым обеспечивая командную работу хирурга и медсестры, их взаимодействие, способность операционной сестры предугадывать потребности хирурга. Это важное дополнение к полному многоролевому командному тренингу также может быть использовано для индивидуального тренинга хирурга и операционной сестры в паре.
Опция доступна для модулей:
- Аппендэктомия
- Гистерэктомия
- Лобэктомия
Опция виртуальной реальности
Новая опция виртуальной реальности, при которой, надев специальные очки, обучаемый погружается в 3D-среду виртуальной операционной с присутствием операционной бригады, реалистичной обстановкой и расположением оборудования. Персонал операционной воссоздает рабочую атмосферу.


Доступна для модулей:
- Холецистэктомия (скоро)
- Аппендэктомия
- Паховая грыжа
- Дистальная резекция желудка
- Гистерэктомия (скоро)
Варианты комплектации
|
SXLM3 |
Симулятор ЛапМентор в комплекте с модулем «Базовые лапароскопические навыки» + 1 модуль на выбор |
|
SXLM3MF |
Симулятор ЛапМентор в комплекте с базовыми модулями + 4 модуля на выбор |
|
SXLM3ME |
Симулятор ЛапМентор в комплекте с базовыми модулями + 8 модулей на выбор |
|
SXLM3MА |
Симулятор ЛапМентор с полным набором модулей (кроме опции VR и командного тренинга) |
Опции командного тренинга
|
SXLM-TT1 |
Пакет «Обучение операционной бригады», комплектация 1: портативный симулятор ЛапМентор Экспресс, установленный на пьедестале |
|
SXLM-TT2 |
Пакет «Обучение операционной бригады», комплектация 2: портативный симулятор ЛапМентор Экспрес (для индивидуальной работы включен только модуль «Базовые лапароскопические навыки», дополнительные модули заказываются отдельно), включает ноутбук |
|
SXLM-TT3 |
Пакет «Обучение операционной бригады», комплектация 3: портативный симулятор ЛапМентор Экспрес со стойкой, компьютером и сенсорным экраном (для индивидуальной работы включен только модуль «Базовые лапароскопические навыки», дополнительные модули заказываются отдельно) |
*обязательное наличие оригинального модуля
Опции виртуальной реальности
|
SXLM-MVR |
Модуль с опцией "Виртуальная реальность" (с очками виртуальной реальности) |
Опции Проктора и Выбора операционного инструментария
|
SXLM3-PROCTORM |
Опция "Режим Проктора и Выбора операционного инструментария" для 3 модулей: Аппендэктомия, Лобэктомия, Гистерэктомия (наличие основного модуля обязательно) *доступно только для НОВЫХ, заказываемых симуляторов |
|
SXLM3-ap-PROCTORM |
Пакет дополнений опцией "Режим Проктора и Выбора операционного инструментария" для 3 модулей: Аппендэктомия, Лобэктомия, Гистерэктомия (наличие основного модуля обязательно) *доступно только для СУЩЕСТВУЮЩИХ клиентов, ранее не закупвшим модули с функцией Проктора |
Базовые модули
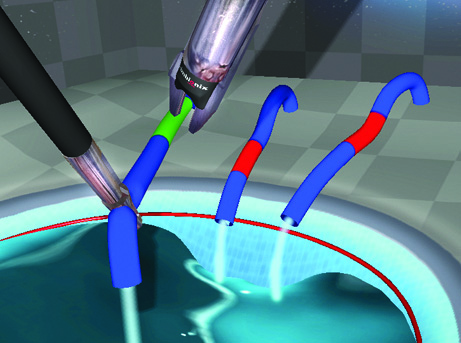
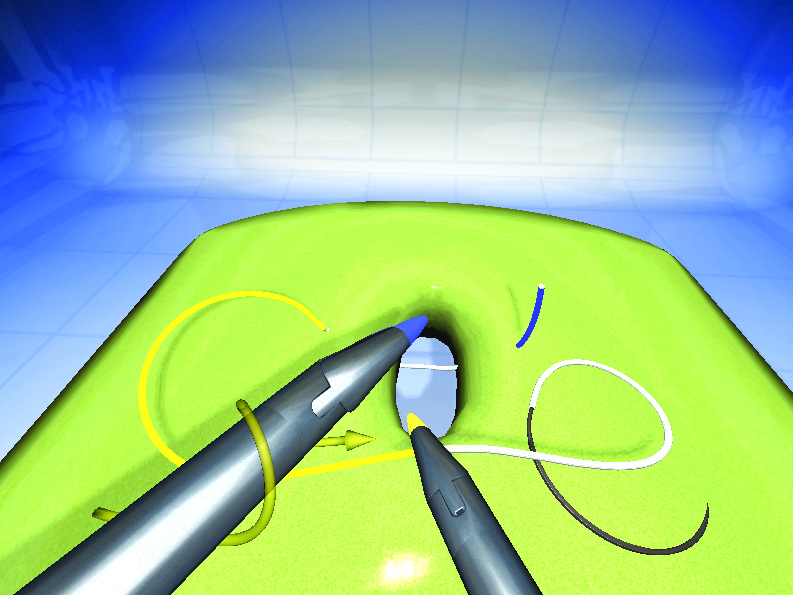
- Базовые лапароскопические навыки
- Важнейшие лапароскопические навыки
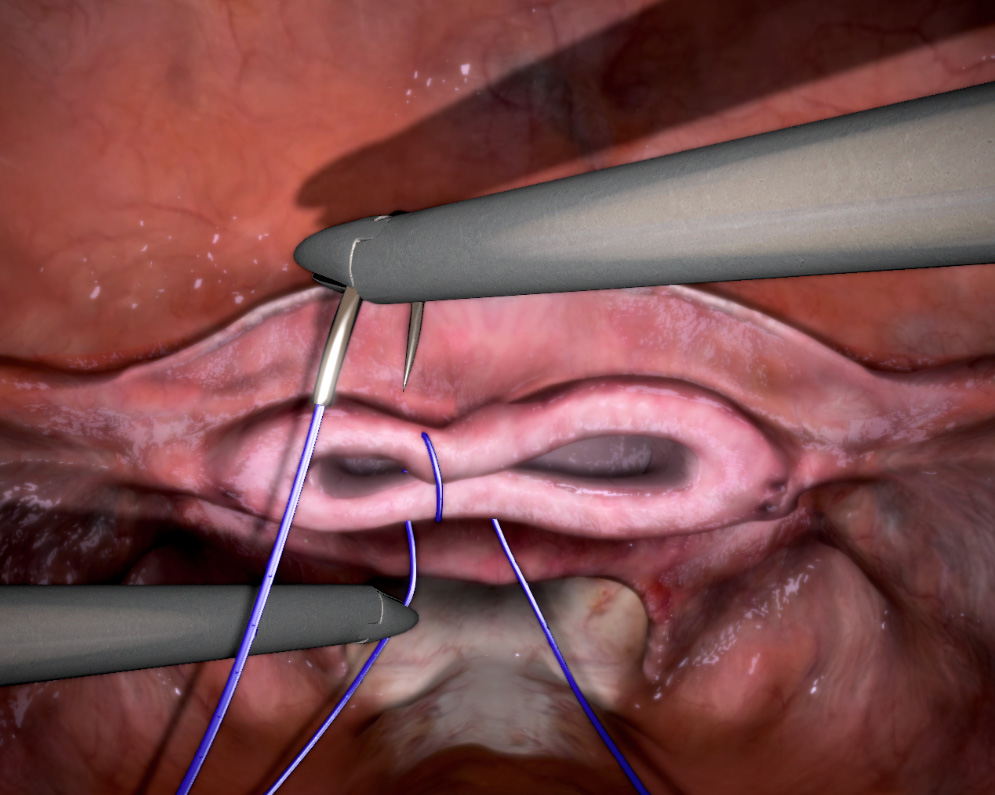
- Базовые навыки наложения швов
- Углубленные навыки наложения швов
- Навыки работы с лапароскопической камерой
Хирургия
- Аппендэктомия
- Лапароскопическая холецистэктомия
- Паховая грыжа
- Послеоперационная грыжа
- Холангиография
- Фундопликация по Ниссену
Бариатрическая хирургия
Колопроктология
Торакальная хирургия
Гинекология
- Важнейшие навыки в гинекологии
- Гистерэктомия
- Ушивание культи влагалища
- Ушивание матки после миомэктомии
Урология
Medical Students Laparoscopic Basic Skills Training:
A Model Based on Minimum Repetition
Rafael dos Santos Mazzuca, Patricia Riberio dos Santos, Thamyres Zanirati, Leonardo Hekman D’avila, Thiago Bozzi de Araujo, Leonardo Totti Cavazolla
Instituto Simutec, Porto Alegre, Rio Grande do Sul, Brazil
INTRODUCTION: The practice of video surgery requires motor skills to perform the procedure. This kind of abilities ranging from notions of depth to understanding of the fulcrum effect. Training of medical students in basic laparoscopic activities plays an important role in medical education. It exposes future physicians to laparoscopy and increases dexterity for those who will specialize in surgery. It’s important to have a defined and structured curriculum for better skills development. In this study, we aimed to quantitatively compare the acquisition and improvement of surgical skills between free training and minimum-repetition based models of training.
MATERIAL AND METHODS: Two groups (G1 and G2) of 37 students each were assessed after completing the basic skills module in the Simbionix LAP Mentor laparoscopy simulator at instituto Simutec, Porto Alegre, Rio Grande do Sul, Brazil. The group that performed a free training without a minimum number of repetitions required was designated G1, while the group that performed a minimum-repetition based model in which activity should be repeated at least 20 times before advancing to the next one, was designated G2. Four activities were assessed: Camera manipulation, hand-eye coordination, clipping, and cutting activity A, B, C and D. Activities scoring data were evaluated based on quantitative objectives. The data were analyzed using the software IBM ® SPSS ® statistics.
RESULTS: The G2 group showed an increase in the number of sessions trained when compared to G1, being significantly higher when analyzed tasks A,C and D (p<0.05). G2 also obtained better results, when efficiency was analyzed, in relation to G1, suggesting a significant improvement when completing the tasks A,C, and D (p<0.05).
CONCLUSION: The simulator with virtual reality allows quantitative measurements of the skills needed to perform a video surgery. From the results, it is possible to affirm that the students that practice with the objective to reach the minimum repetitions required per session (G2) has a more efficient training session than those students that did it freely (G1). In addition, students that have minimum repetitions as an objective to reach, trained more sessions than students with free training, making them more skillful and efficient in their activities. The training based on a minimum number of repetitions can be an alternative capable of improving students’ efficiency and may better prepare them to perform video laparoscopy surgery.
Validation of a virtual reality laparoscopic appendicectomy simulator: a novel process using cognitive task analysis
Sandeep Krishan Nayar, Liam Musto, Roland Fernandes, Rasiah Bharathan
Published: Irish Journal of Medical Science, 2018 Nov 19. doi: 10.1007/s11845-018-1931-x
BACKGROUND: Virtual reality (VR) simulation is a vital component of surgical training with demonstrated improvements in surgical quality and clinical outcome.
AIMS: To validate the LAP Mentor (Simbionix™) laparoscopic appendicectomy (LA) VR simulator with inclusion of a novel tool, Cognitive Task Analysis (CTA).
METHODS: Thirty-two novices and nine experienced surgeons performed two simulated LAs. An expert-consensus questionnaire guided face validity assessment. Content validity was assessed using CTA-derived questions encompassing eight operative steps and four decision points. Construct validity was evaluated using dexterity metrics, masked assessment of surgical quality using the OSATS global rating scale, and mental workload from two validated tools: the NASA-TLX and SMEQ. Ten novices performed eight further LAs for learning curve assessment.
RESULTS: Face validity was demonstrated across all domains. Considering content validity, the essential technical and non-technical steps were evident. The experienced group performed the procedure quicker (median time 361 vs. 538 s, P = 0.0039) with fewer total movements (426 vs. 641, P < 0.0001) and shorter idle time (131 vs. 199 s, P = 0.0006). This correlated with higher OSATS scores (median 33.5 vs. 22.2, P < 0.0001) and lower mental demand (NASA-TLX: 9.0 vs. 13.75, P = 0.012; SMEQ: 60 vs. 80, P = 0.0025), indicating construct validity. Learning curve data showed statistically significant improvements after the 7th session for procedure time, total movements and idle time, which correlated with reduction in mental demand.
CONCLUSIONS: The LAP Mentor demonstrates face, content and construct validity for LA; thus, it can be used as an effective tool in surgical training. Task repetition leads to achievement of expert benchmarks.
The Heidelberg VR Score: development and validation of a composite score for laparoscopic virtual reality training
Mona W. Schmidt, Karl‑Friedrich Kowalewski, Marc L. Schmidt, Erica Wennberg, Carly R. Garrow, Sang Paik, Laura Benner, Marlies P. Schijven, Beat P. Muller‑Stich, Felix Nickel
Published in Surgical Endoscopy, October 2018
DOI: 10.1007/s00464-018-6480-x
INTRODUCTION: Virtual reality (VR-)trainers are well integrated in laparoscopic surgical training. However, objective feedback is often provided in the form of single parameters, e.g., time or number of movements, making comparisons and evaluation of trainees’ overall performance difficult. Therefore, a new standard for reporting outcome data is highly needed. The aim of this study was to create a weighted, expert-based composite score, to offer simple and direct evaluation of laparoscopic performance on common VR-trainers.
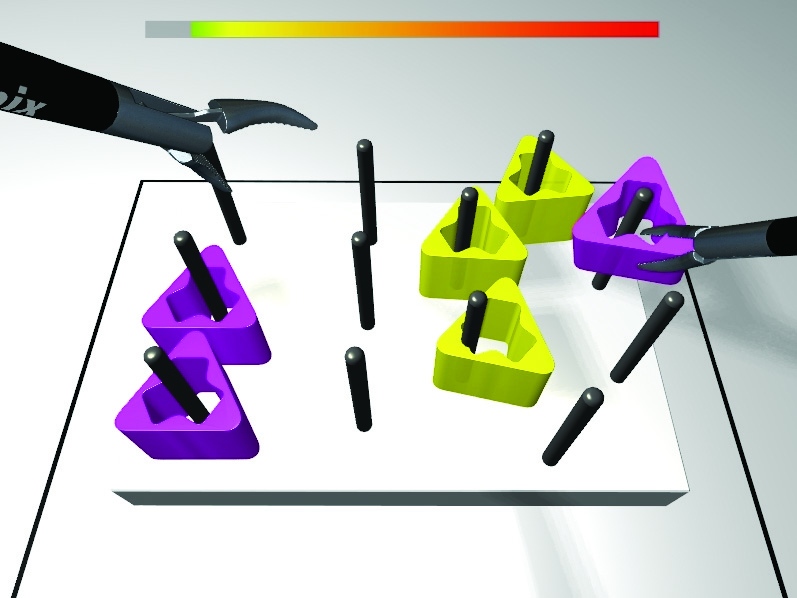
MATERIALS AND METHODS: An integrated analytic hierarchy process-Delphi survey was conducted with 14 international experts to achieve a consensus on the importance of different skill categories and parameters in evaluation of laparoscopic performance. A scoring algorithm was established to allow comparability between tasks and VR-trainers. A weighted composite score was calculated for basic skills tasks and peg transfer on the LapMentor™ II and III and validated for both VR-trainers.
RESULTS: Five major skill categories (time, efficiency, safety, dexterity, and outcome) were identified and weighted in two Delphi rounds. Safety, with a weight of 67%, was determined the most important category, followed by efficiency with 17%. The LapMentor™-specific score was validated using 15 (14) novices and 9 experts; the score was able to differentiate between both groups for basic skills tasks and peg transfer (LapMentor™ II: Exp: 86.5 ± 12.7, Nov. 52.8 ± 18.3; p < 0.001; LapMentor™ III: Exp: 80.8 ± 7.1, Nov: 50.6 ± 16.9; p < 0.001).
CONCLUSION: An effective and simple performance measurement was established to propose a new standard in analyzing and reporting VR outcome data—the Heidelberg virtual reality (VR) score. The scoring algorithm and the consensus results on the importance of different skill aspects in laparoscopic surgery are universally applicable and can be transferred to any simulator or task. By incorporating specific expert baseline data for the respective task, comparability between tasks, studies, and simulators can be achieved.
Simulation-Based Testing of Pager Interruptions During Laparoscopic Cholecystectomy
Joseph A.Sujka, MD, Karen Safcsak, RN, Indermeet S.Bhullar, MD, FACS, William S.Havron III, MD, FACS
Published: Journal of Surgical Education, Volume 75, Issue 5, September–October 2018, Pages 1351-1356
https://doi.org/10.1016/j.jsurg.2018.01.012
OBJECTIVE: To determine if pager interruptions affect operative time, safety, or complications and management of pager issues during a simulated laparoscopic cholecystectomy.
DESIGN: Twelve surgery resident volunteers were tested on a Simbionix Lap Mentor II simulator. Each resident performed 6 randomized simulated laparoscopic cholecystectomies; 3 with pager interruptions (INT) and 3 without pager interruptions (NO-INT). The pager interruptions were sent in the form of standardized patient vignettes and timed to distract the resident during dissection of the critical view of safety and clipping of the cystic duct. The residents were graded on a pass/fail scale for eliciting appropriate patient history and management of the pager issue. Data was extracted from the simulator for the following endpoints: operative time, safety metrics, and incidence of operative complications. The Mann-Whitney U test and contingency table analysis were used to compare the 2 groups (INT vs. NO-INT).
SETTING: Level I trauma center; Simulation laboratory.
PARTICIPANTS: Twelve general surgery residents.
RESULTS: There was no significant difference between the 2 groups in any of the operative endpoints as measured by the simulator. However, in the INT group, only 25% of the time did the surgery residents both adequately address the issue and provide effective patient management in response to the pager interruption.
CONCLUSION: Pager interruptions did not affect operative time, safety, or complications during the simulated procedure. However, there were significant failures in the appropriate evaluations and management of pager issues. Consideration for diversion of patient care issues to fellow residents not operating to improve quality and safety of patient care outside the operating room requires further study.
Все тезисы можно посмотреть здесь
- Воронежский государственный медицинский университет им. Н.Н. Бурденко
- Ингушский государственный университет
- Иркутская областная клиническая больница
- Московский государственный медико-стоматологический университет имени А.И. Евдокимова
- Московский областной научно-исследовательский клинический институт им. М. Ф. Владимирского
- Научный центр акушерства, гинекологии и перинатологии имени академика В.И. Кулакова
- Национальный медицинский исследовательский центр фтизиопульмонологии и инфекционных заболеваний
- Национальный медицинский исследовательский центр хирургии им. А.В. Вишневского
- Оренбургский государственный медицинский университет
- Первый Московский государственный медицинский университет имени И.М. Сеченова
- Российский национальный исследовательский медицинский университет имени Н.И. Пирогова
- Ростовский государственный медицинский университет
- Российский университет дружбы народов
- Рязанский государственный медицинский университет имени академика И.П. Павлова
- Санкт-Петербургский государственный педиатрический медицинский университет
- Саратовский государственный медицинский университет им. В.И. Разумовского
- Северо-Западный государственный медицинский университет имени И. И. Мечникова
- Сибирский государственный медицинский университет
- Ханты-Мансийская государственная медицинская академия
